Abdominal Aortic Aneurysm
Introduction:
Abdominal aortic aneurysm (AAA) refers to dilation of the aortic vessel. Most AAAs are asymptomatic until they rupture. Atherosclerosis is highly linked as an underlying cause of AAA. Atherosclerosis places increased pressure on the vessel, leading to enlargement. There is a high mortality among individuals with an AAA rupture. Therefore, it is crucial to identify patients at risk for a ruptured AAA immediately.
Risk factors associated with AAA include:
Signs & Symptoms of a non-ruptured vessel:
Pain Description:
Signs & Symptoms of a ruptured vessel:
Referral Patterns
Special Tests
Presence of signs and symptoms of an AAA requires immediate medical attention.
References
Besiardins, B., Dill, K E, Flamm, SD, Francois, CJ, Gerhard-Herman, MD, Kalva, SP, Mansour, MA, & Mohler, ER. (2013). Acr appropriateness criteria pulsatile abdominal mass, suspected abdominal aortic aneurysm. Int J Cardiovasc, 29(1), 177-183. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles /PMC3550697/
Booher, AM and KA Eagle. (2011). "Diagnosis and management issues in thoracic aortic aneurysm." Am Heart J 162(1), 38-46.
Dobrin PB. (1989). Pathophysiology and pathogenesis of aortic aneurysms. Current concepts. Surg Clin North Am, 69(4),687–703.
Forsdahl SH, Singh K, Solberg S, Jacobsen BK. 2009. Risk factors for abdominal aortic aneurysms: a 7-year prospective study: the Tromso Study, 1994-2001. Circulation, 119, 2202-2208
Goodman, MBA, PT, C. C., & Snyder, MN, RN, OCN, T. E. (2007). Differential Diagnosis PHYSICAL THERAPISTS Screening for Referral (4thth ed.). St. Louis, MO:Saunders Elsevier.
Lederle, F., & Simel, D. (1999). The rational clinical examination. does this patient have abdominal aortic aneurysm?. JAMA, 281(1), 77-82.
Reed D, Reed C, Stemmermann G, et al. (1992) Are aortic aneurysms caused by atherosclerosis? Circulation, 85(1), 205–211. Retrieved from http://circ.ahajournals.org/content/85/1/205.long
Singh K, Bonaa KH, Jacobsen BK, Bjork L, Solberg S. (2001). Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study : The Tromso Study. Am J Epidemiol, 154(3):236.
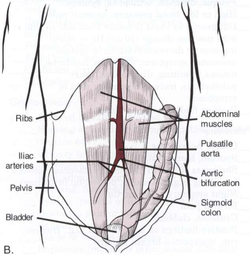
Image retrieved from: http://www.sirweb.org/patients/abdominal-aortic-aneurysms/
Abdominal aortic aneurysm (AAA) refers to dilation of the aortic vessel. Most AAAs are asymptomatic until they rupture. Atherosclerosis is highly linked as an underlying cause of AAA. Atherosclerosis places increased pressure on the vessel, leading to enlargement. There is a high mortality among individuals with an AAA rupture. Therefore, it is crucial to identify patients at risk for a ruptured AAA immediately.
Risk factors associated with AAA include:
- Age over 65 years old
- Men
- Smoking
- Hypertension
- Family history
- History of intermittent claudication
- History of diminished or absent peripheral pulses
- Congenital malformation
- Vasculitis
- Wait/hip ratio
- Systolic blood pressure (in women)
Signs & Symptoms of a non-ruptured vessel:
- Pulsating mass in the abdomen
- Abdominal and/or back pain
Pain Description:
- Sharp, intense, severe or knife-like
- Tearing
Signs & Symptoms of a ruptured vessel:
- Sudden, severe chest pain with a tearing sensation
- Pain in the neck, low back, between the scapulae, abdomen, or posterior thigh
- Pain unrelieved by a change in position
- Pulsating abdominal mass
- Cold, absent lower extremity pulse, or blood pressure change
- Ecchymoses in the flank and perianal area
- Lightheadedness and nausea
Referral Patterns
- Groin and flank pain
- Chest
- Scapulae
- Posterior thighs
Special Tests
- Palpation of arterial pulses has shown to be safe. Normal width over 50 years old is less than 3 centimeters wide. Palpation should occur with the patient in supine, hook lying. Palpate below the umbilicus with an index finger on each side of the aortic vessel. Positive predictive value is >43% for an AAA greater than 3 cm. Sensitivity values range from 29-76% depending on the size of the enlargement.
- Listen for bruits with stethoscope
- Monitor vitals
- US and CT by physician
Presence of signs and symptoms of an AAA requires immediate medical attention.
References
Besiardins, B., Dill, K E, Flamm, SD, Francois, CJ, Gerhard-Herman, MD, Kalva, SP, Mansour, MA, & Mohler, ER. (2013). Acr appropriateness criteria pulsatile abdominal mass, suspected abdominal aortic aneurysm. Int J Cardiovasc, 29(1), 177-183. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles /PMC3550697/
Booher, AM and KA Eagle. (2011). "Diagnosis and management issues in thoracic aortic aneurysm." Am Heart J 162(1), 38-46.
Dobrin PB. (1989). Pathophysiology and pathogenesis of aortic aneurysms. Current concepts. Surg Clin North Am, 69(4),687–703.
Forsdahl SH, Singh K, Solberg S, Jacobsen BK. 2009. Risk factors for abdominal aortic aneurysms: a 7-year prospective study: the Tromso Study, 1994-2001. Circulation, 119, 2202-2208
Goodman, MBA, PT, C. C., & Snyder, MN, RN, OCN, T. E. (2007). Differential Diagnosis PHYSICAL THERAPISTS Screening for Referral (4thth ed.). St. Louis, MO:Saunders Elsevier.
Lederle, F., & Simel, D. (1999). The rational clinical examination. does this patient have abdominal aortic aneurysm?. JAMA, 281(1), 77-82.
Reed D, Reed C, Stemmermann G, et al. (1992) Are aortic aneurysms caused by atherosclerosis? Circulation, 85(1), 205–211. Retrieved from http://circ.ahajournals.org/content/85/1/205.long
Singh K, Bonaa KH, Jacobsen BK, Bjork L, Solberg S. (2001). Prevalence of and risk factors for abdominal aortic aneurysms in a population-based study : The Tromso Study. Am J Epidemiol, 154(3):236.
Image retrieved from: http://www.sirweb.org/patients/abdominal-aortic-aneurysms/
